 Date: 2016-09-06 11:08:31
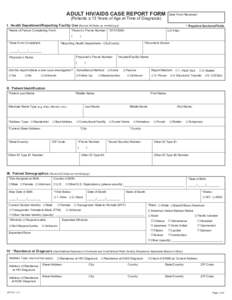
| |  ADULT HIV/AIDS CASE REPORT FORM (Patients ≥ 13 Years of Age at Time of Diagnosis) Date Form Received: I. Health Department/Reporting Facility Use (Record All Dates as mm/dd/yyyy) ADULT HIV/AIDS CASE REPORT FORM (Patients ≥ 13 Years of Age at Time of Diagnosis) Date Form Received: I. Health Department/Reporting Facility Use (Record All Dates as mm/dd/yyyy)
Add to Reading ListSource URL: publichealth.lacounty.govDownload Document from Source Website File Size: 1,41 MBShare Document on Facebook
|