 Date: 2017-12-15 14:18:41
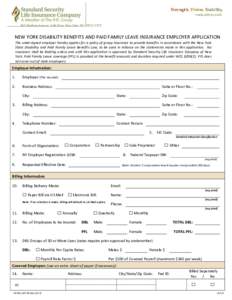
| |  NEW YORK DISABILITY BENEFITS AND PAID FAMILY LEAVE INSURANCE EMPLOYER APPLICATION The undersigned employer hereby applies for a policy of group insurance to provide benefits in accordance with the New York State Disabili NEW YORK DISABILITY BENEFITS AND PAID FAMILY LEAVE INSURANCE EMPLOYER APPLICATION The undersigned employer hereby applies for a policy of group insurance to provide benefits in accordance with the New York State Disabili
Add to Reading ListSource URL: www.sslicny.comDownload Document from Source Website File Size: 912,07 KBShare Document on Facebook
|